
Frozen Shoulder
Frozen Shoulder is characterised by increasing pain and then increasing stiffness in the shoulder
Do you have a Frozen Shoulder?
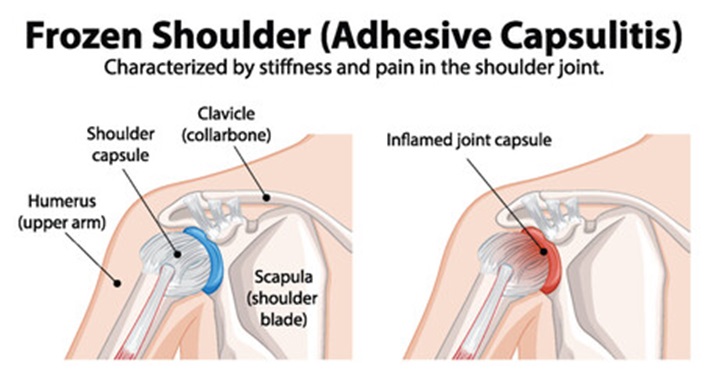
Anatomy and Pathology of Frozen Shoulder
What is a frozen shoulder?
Frozen shoulder, or “primary frozen shoulder” is a condition associated with severe shoulder pain without any preceding trauma or strain on the shoulder, and limitation of shoulder mobility in all directions. It affects 2-5% of the general population, is more common in women and the prevalence increases to 20% in people with diabetes. Other medical conditions such as thyroid disease, adrenal disease, cardiopulmonary disease and hyperlipidemia are associated with the incidence of frozen shoulder. Frozen shoulder starts insidiously and recent research indicates that our body’s inflammatory and immunological response may trigger inflammation of the joint capsule’s synovial lining, eventually leading to thickening and shortening of the capsular structure.
People with this condition present with pain localised to the shoulder/upper arm, pain with movement, night pain with difficulty sleeping on the painful side, and marked limitation of the shoulder movement in reaching out to the side, in lifting the arm forward and reaching behind the back. The average duration for this condition to resolve without any treatment can range from 1 to 3.5 years but in some individuals can be substantially longer. This condition has three phases which can overlap:
- Painful phase (lasting 2-9 months)
- Stiff phase (lasting 4-12 months) and
- Recovery (lasting 5-24 months).
Diagnosis of a frozen shoulder requires a thorough assessment and the exclusion of other medical conditions that may have similar symptoms.
Treatment options
The shoulder pain can be quite debilitating for some people and pain management with medications is recommended in the painful phase of the condition. There is good evidence that in people who have symptoms for less than a year, corticosteroid injection given in the shoulder joint is effective in pain relief for 3-6 months. Physiotherapy treatment, which includes gentle exercises and stretches, can also improve shoulder mobility and function. A combination of corticosteroid injection and physiotherapy treatment is more effective in decreasing pain and improving function.
Other Treatment options include hydrodilatation and capsular release. In hydrodilatation, a needle is placed into the joint and either corticosteroid or sterile saline is injected into the joint to stretch the capsule. This procedure is done under ultrasound guidance. There is evidence that this procedure along with corticosteroid injection is effective for pain relief for a short period. There is no conclusive evidence for its efficacy as a stand-alone treatment. Capsular release is a surgical procedure done under general anaesthesia and again does not have conclusive evidence as to whether it is superior to conservative treatment.
