
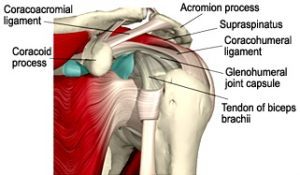
The shoulder is an unstable joint because of the limited bony contact. The shoulder therefore relies heavily on muscles and ligaments to hold the joint together.
The shoulder is an unstable joint because of the limited bony contact. The shoulder therefore relies heavily on muscles and ligaments to hold the joint together.
Most dislocations (≈90%) will dislocate anteriorly i.e. the humeral head will pop out the front. The arm is typically out to the side when this happens, with the hand raised above the head. It can happen because of trauma which pushes the hand backwards, or an external force which pushes the shoulder forward.

Most dislocations (≈90%) will dislocate anteriorly i.e. the humeral head will pop out the front. The arm is typically out to the side when this happens, with the hand raised above the head. It can happen because of trauma which pushes the hand backwards, or an external force which pushes the shoulder forward.

Adhesive Capsulitis (also known as “Frozen Shoulder”) is a condition which is characterised by severe pain and loss of motion of the shoulder joint. It is more common in women, in those in their 6th decade, and can be associated with diabetes and duputryn’s contractures.
The natural history is a 2 year course which is defined by 3 distinct phases. Phase 1 (‘Freezing) is typified by pain and progressive loss of movement and lasts from six weeks to nine months. Phase 2 (“Frozen”) presents with more loss of movement than pain and can last from seven weeks to nine months. Phase 3 (“Thawing”) involves the gradual resolution of range of movement and involves very little pain.
Treatment options include early cortico-steroid injection (within the first 3 months of Phase 1). Physiotherapy may include gentle range of motion stretches in this phase. Treatment in Phase 2 and 3 may be more directed towards mobilisations and a continuation of stretches. Care should be taken not to increase pain during the treatment. Click here for our you tube video on Frozen shoulder.
When your shoulder dislocates with your arm out in front of you or out to the side, strain is placed upon the capsule or the labrum (the cartilage which deepens the shoulder socket) at the front of the shoulder. Too much strain on this capsule / labrum will cause a tear. This tear is called a Bankart lesion and may affect either the capsule or the labrum. A large percentage of people (≈90%) who dislocate their shoulders will either damage the labrum of the shoulder capsule.
 Patients who are younger tend to tear in the labrum, while older patients (over the age of 40 years) tend to tear the capsule or muscles. The damage to the labrum may be one reason that younger people tend to have more recurrent dislocations than older people.
Patients who are younger tend to tear in the labrum, while older patients (over the age of 40 years) tend to tear the capsule or muscles. The damage to the labrum may be one reason that younger people tend to have more recurrent dislocations than older people.
 The presence of a Bankart lesion affects the stability of your shoulder and may alter the centre of rotation of your humerus. This can cause pain or instability.
The presence of a Bankart lesion affects the stability of your shoulder and may alter the centre of rotation of your humerus. This can cause pain or instability.
Bony Bankart lesions occur during a shoulder dislocation. Whereas other Bankart lesions involve the capsule or labrum (cartilage which deepens the shoudler socket), a bony bankart lesion, typically involves a chip of bone being removed from the anterior-inferior part of the shoulder socket (glenoid). These fractures can vary in size, and treatment of the bony bankart lesion is dependent upon how big the chip of bone is.
 X-rays are the best way of detecting a bony bankart lesion. Because of the position of the fracture, they are not visible in standard AP or alteral views. Detection of the bonyt bankart lesion is best undertaken with a Westpoint view, in which the patient lis on their stomach with their arm out to the side. The camera is positioned at an angle to get the best view of the fracture
X-rays are the best way of detecting a bony bankart lesion. Because of the position of the fracture, they are not visible in standard AP or alteral views. Detection of the bonyt bankart lesion is best undertaken with a Westpoint view, in which the patient lis on their stomach with their arm out to the side. The camera is positioned at an angle to get the best view of the fracture
A Frozen shoulder (sometimes called ‘Adhesive Capsulitis’) is a term for a shoulder that has decreased movement because of stiffness and changes in the structure of the joint capsule. It can occur without any trauma (primary) or following injury (secondary). It is more common in women than men, and most common in people in their 6th decade. There also appears to be some links with dupuytren contractures and diabetes. There appears to be no relationship with hand dominance.
A frozen shoulder typically has four phases.
1. An initial painful phase characterised by pain in the shoulder which typically will prevent you from sleeping. There is not much noticeable limitation in the range of movement
2. The pain continues in your shoulder but you will start to notice a decrease in the range of motion in your shoulder, both actively (the movement you can make with your shoulder) and passively (the movement somebody else can make with your shoulder when the muscles are relaxed)
3. In the third phase the pain in the shoulder starts to decrease, but there still remains considerable limitation in the range of movement in your arm.
4. The fourth stageis the resolution stage and both the pain and the stiffness resolve until your shoulder is back to about 95% better
A full resolution typically takes between 12 and 24 months and while people commonly regain all their function, sometimes limitations in the shoulder range of movement remains.
 A Hill Sach’s lesion is a dent in your humeral head. This occurs during a dislocation beccause the bone in the humeral head (the ball) is softer than the hard bone of the glenoid (the socket). In an anterior dislocation, the humeral slides forward and the soft bone of the back of the shoulder butts against the hard bone of the front of the glenoid, causing an indentation in the bone. When a posterior dislocation / subluxation occurs, the humeral head slides posteriorly and the front of the humeral head butts against the posterior part of the glenoid. This causes an indentation in the front of the humeral head which is called a reverse Hill Sach’s lesion.
A Hill Sach’s lesion is a dent in your humeral head. This occurs during a dislocation beccause the bone in the humeral head (the ball) is softer than the hard bone of the glenoid (the socket). In an anterior dislocation, the humeral slides forward and the soft bone of the back of the shoulder butts against the hard bone of the front of the glenoid, causing an indentation in the bone. When a posterior dislocation / subluxation occurs, the humeral head slides posteriorly and the front of the humeral head butts against the posterior part of the glenoid. This causes an indentation in the front of the humeral head which is called a reverse Hill Sach’s lesion.
 Hill Sach’s lesions are only evident on X-Ray. They require a special angulation of the X-Ray machine. This is called a Stryker notch view, because of the notch seen in your humeral head
Hill Sach’s lesions are only evident on X-Ray. They require a special angulation of the X-Ray machine. This is called a Stryker notch view, because of the notch seen in your humeral head
One of the main causes of shoulder pain is an imbalance in the muscle strength of the rotator cuff muscles around your shoulder. The four muscles of the rotator cuff work together to stabilise the humeral head in the shoulder socket. If there is an imbalance, this can result in pain
 The shoulder is an unstable joint because of the limited bony contact. The shoulder therefore relies heavily on muscles and ligaments to hold the joint together.
The shoulder is an unstable joint because of the limited bony contact. The shoulder therefore relies heavily on muscles and ligaments to hold the joint together.
Most dislocations (≈90%) will dislocate anteriorly i.e. the humeral head will pop out the front. The arm is typically out to the side when this happens, with the hand raised above the head. It can happen because of trauma which pushes the hand backwards, or an external force which pushes the shoulder forward.
eople with anterior instability typically feel nervous with their arm stretched out to the side, or above the head. They may also feel pain in the front of the shoudler in these positions. Bankart lesions, Hill Sach Lesions commonly occur in an anterior dislocation. Subluxations can also occur in an anterior direction.
 The research is based upon the fact that anterior shoulder dislocations commonly occur in a position where your arm is outstretched with your hand rotated upwards. In this position the capsule at the front of your shoulder is exposed. The brace acts to limits the amount of movement that your arm can move, and therefore decreases the risk of you suffering from another dislocation.
The research is based upon the fact that anterior shoulder dislocations commonly occur in a position where your arm is outstretched with your hand rotated upwards. In this position the capsule at the front of your shoulder is exposed. The brace acts to limits the amount of movement that your arm can move, and therefore decreases the risk of you suffering from another dislocation.
It is also proposed that the brace helps to increase the proprioception around the joint by increasing the compression on the skin receptors and thus make up for the fact that receptors in the ligaments and muscles might be damaged from the injury. Research into this is continuing.
The shoulder is an unstable joint because of the limited bony contact. The shoulder therefore relies heavily on muscles and ligaments to hold the joint together.
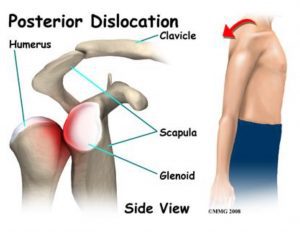
Some dislocatiosn occur posteriorly i.e. the humeral head will pop out the back. The arm is typically in front o fthe body and forced backwards, or force across the body (like if you were trying to hug yourself). In people who have increaed laxity in their shoulders, the shoulder can dislocate posteriorly with minor trauma such os pushing open a heavy door, or doing press-ups or CPR.
People with posterioinstability typically feel nervous when their arm is drawn across their body with the hand twisted down. They may also feel pain or apprehension when pushing open a heavy door. Reverse Bankart lesions or Reverse Hill Sachs lesions can occur during a posterior dislocation. Subluxations can also occur in an posterior direction.
Push-ups are typically used to strength Pectoralis Major, the large chest muscle that lies across the front of your chest. Research into the use in increased strength of this muscle remains variable.
Some propose that increased strength of Pectoralis Major draws the humeral head forward and increases the instability of the shoulder. Other people propose that any strength around the shoulder is good for it, and will prescribe push-ups as part of the strengthening regime.
At Flawless Motion, we believe that push-ups may assist in shoulder strengthening, but should only be incorporated at the end stage of rehabilitation. In this manner, they may provide a pre-cursor to “push-up claps” which increase the speed of activation and co-ordination around the joint.

Shoulder impingement refers to compression (or impingement) of tendons (and/or bursa) around the shoulder. There are three different classifications.
Primary impingement refers to compression of the subacromial bursa and/or supraspinatus tendon due to decreased space under the acromial arch. This may be due to changes in the under surface of the acromion, or calcific deposits in the supraspinatus tendon to name a few. Patients will present with anterior shoulder pain and will have changes visible on X-Ray.
Secondary impingement refers to inflammation of the tendons and/or bursa under the acromial arch due to decreased stability of wither the Glenohumeral joint, or scapulothoracic joint. The resulting increased movement increases compression on the sub-acromial bursa and supraspinatus tendon.
The biceps tendon can also be involved and irritated. Patients will present with anterior shoulder pain and are typically under the age of 35 years.
Internal impingement is impingement at the posterior shoulder of the supraspinatus and infraspinatus tendon. This can occur when the humeral head slides forward and the elbow extends, the pinching the posterior structures. Patients present with posterior shoulder pain which is worse when reaching behind them.
Scapular instability is a term that indicates that you have increased movement or decreased control of your scapular.
The scapula relies heavily on muscel control as the only ligamentous fixation is via your acromioclavicular joint (ACJ) and your collar bone (clavicle). Thus scapular instability commonly occurs when the muscles around your scapula are not strong enough to hold onto the scapula bone.
Increased movement in your scapula can result in pain in your shoulder joint. This is because the foundation on which the shoulder socket is placed is moving and therefore pinching of tendons or bursa around your shoulder can result. It is kind of like a house that is built on a sandy soil. Because the foundations of the house are unstable and moving around, cracks and damage can appear in the walls and floors of the house. In a similar way, scapular instability can contribute to shoulder instability.
Your therapist will commonly prescribe exercises to strengthen themuscles around your scapula. These exercises may include push-ups, prone holds, side holds, seated row to name a few. Check out some exercises for Serratus anterior on this website to give you a few new ideas.
Shoulder proprioception refers to the ability of the muscles, ligament, skin and joint capsule to detect movement, force, or activity. Muscle receptors detect stretch on the muscle. Tendon receptors alsodetect the amount of pull on the tendon. Joint receptors detect the amount of stretch or compression on the capsule. Together these proprioceptors act to send information to the brain regarding the position, movement or level of activation in muscles around your shoulder. Without this information, you would not be able to tell the position of your shoulder, whether your muscles are working or if you are touching something.
 Proprioception can be decreased in longstanding shoulder injuries, and has been documented in cases of recurrent instability. Some people have proposed that decreased proprioception may result in an increased risk to injury, although there is little evidence to support this.
Proprioception can be decreased in longstanding shoulder injuries, and has been documented in cases of recurrent instability. Some people have proposed that decreased proprioception may result in an increased risk to injury, although there is little evidence to support this.
Your shoulder is held is place by ligaments and muscles. When your shoulder subluxes out of its socket, this is because the ligaments and muscles are lax or ruptured.
When a subluxation occurs, the humeral head slips out of its socket, it slips back in with minimal movement of the arm.
Symptoms include shoulder pain, a ‘dead arm’ or paraesthesia for a short moment in time. When a dislocation occurs the humeral head slips out of the socket, it does not relocate by itself.
A shoulder dislocation requires relocating by external force, commonly performed in a hospital.
Shoulder dislocations are typically very painful, and become increasingly painful if they are not relocated within a short space of time.
The increased muscle spasm can make relocation difficult if the shoulder is not relocated by a health professional (as soon as is practicable).
It is advised that a shoulder X-Ray is undertaken following a dislocation to make sure there is no fracture.
Traumatic shoulder dislocations are very painful, and unfortunately for some patients there is a high rate of recurrence. Most research regarding the recurrence of shoulder dislocations has been undertaken in Scandinavia, and there is little research available on a New Zealand population. However, across all races and cultures, the resrach would suggest that repeated shoulder dislocation is more common in those people who have their first dislocation under the age of 20 years. There is some evidence that wearing a brace after a dislocation will reduce the risk of dislocation.
Research in Scandinavia suggests that there is no evidence to say that exposure to sporting activities increasethe risk of dislocation. However, clinically it would seem that in a New Zelanad population those that play more contact sport re more exposed to possible trauma and thus have a higher incidence of shoulder dislocation
 Around 95% of shoulder dislocations occur in an anterior direction. It is thought that this may be due to weakness in the ligamentous structures in your shoulder or because of the range that your shoulder is exposed to and the position when trauma occurs.
Around 95% of shoulder dislocations occur in an anterior direction. It is thought that this may be due to weakness in the ligamentous structures in your shoulder or because of the range that your shoulder is exposed to and the position when trauma occurs.